
 orcid.org/0000-0002-2777-8707
orcid.org/0000-0002-2777-8707


I am currently editing a publication on recovery modalities and have been reading a lot about various recovery methods. Massage is and intervention that fascinates me, mostly because it has been used for centuries to treat athletes (if you want to read more, go here).
Massage consists of physical manipulation of muscle and connective tissue at a site of injury, inflexibility or soreness mainly to promote recovery and/or reduction of pain. It is very popular not only in sport. In fact, apparently 18 million individuals undergo massage therapy annually in the USA. The effectiveness of massage is contentious if you read recent reviews (or here). However despite the lack of clear information about the physiological effects of massage, it is used intensively in the sporting community due to the reported beneficial effects on perception of pain and general wellbeing. In some preliminary studies I have been involved as well as empirical observations with the athletes and teams I worked with clearly suggest that the “perceived” effectiveness of massage depends a lot on who is administering this form of manual therapy and in my experiences the relationship between the perception of beneficial effect and the quality of the practitioner did not support a strong link with the masseur’s ability but rather supported the link with personality traits/gender and other placebo related aspects.
A very interesting recent paper published by Prof. Tarnopolsy’s lab seems to show some promising effects of massage on inflammatory signaling after exercise-induced muscle damage. This is the first study to my knowledge where muscle biopsies were obtained and whole-genome microarrays were used to screen for expressed genes induced by massage. Biopsies were obtained in 11 young male subjects at rest, immediately after administration of massage to a randomised single leg and after 2.5 hours period of recovery. The subjects acted as their own control as one leg recived massage and the other leg no massage following cycling to exhaustion on a cycle ergometer starting at an intensity of 60% of their predetermined VO2 peak.
Here are the details of the experiment as presented in the methods section.
“The exercise bout consisted of upright cycling exercise on an electrically braked cycle ergometer (Lode Excalibur, Lode) pedalling at a workload calculated to elicit 60% of their predetermined VO2peak for 30 min at a cycling cadence between 70 and 90 rpm. After 30 min, the intensity was in- creased to a workload equivalent to 65%VO2peak for 5min, then dropped back to 60% for 5 min, increased to 70% VO2peak for 5 min, dropped to 60% for 5 min, etc., to a maximum of 85% VO2peak. If 85% VO2peak was attained, then subjects continued with intervals of 85% VO2peak for 2 min followed by 60% VO2peak for 2 min, etc., until subject exhaustion. Test completion was ascertained when subjects were unable to maintain a cycling cadence above 70 rpm.
Immediately after exercise, subjects were allowed to recover for 10 min while massage oil was lightly applied to both quadriceps. Thereafter, a single leg was randomized to receive massage treatment for 10 min from a registered massage therapist. The massage treatment was composed of three types of soft tissue manipulations while the subject remained in the supine position. Treatment was focused on the knee extensors muscles, encompassing a range of pressures and movement patterns typically provided during a therapy session. The treatment consisted of (i) 2 min of effleurage, a light stroking technique delivered with a moderate pressure; (ii) 3 min of petrissage, a firm motion involving compression and subsequent pres- sure release from the muscle; (iii) 3min of slow muscle stripping, con- sisting of repeated longitudinal strokes of ~40 s; and (iv) an additional 2min of effleurage. All members of the study team were blinded as to which leg was massaged, with the exception of the massage therapist. After massage, the subjects rested for 10min and a muscle biopsy was obtained from the vastus lateralis of each leg (0 hours). Two and a half hours later (3 hours after the cessation of the exercise bout), a biopsy was again obtained from each leg (2.5 hours).”
The results were quite interesting. First, despite the fact that the model used should not produce large muscle damage, it was enough to disrupt a large number of muscle fibers. Muscle metabolites were shown not to be affected by massage. Massage had no effect on muscle lactate levels and glycogen levels measured immediately after massage or 2.5h later. Furthermore, no significant effects were seen in anabolic signaling (phopshorylation of Akt, mTOR, GSK-3a and GSK-3b was not changed by massage).
Muscle from the massaged leg had larger FAK and ERK1/2 phopshorylation immediately after massage, showing the impact of the mechanical stimulation produced by massage.
The most interesting findings related to the increase in the in MAPK-related signaling proteins 2.5 hours after massage, suggesting an augmentation of mitochondrial biogenesis signaling with massage therapy.
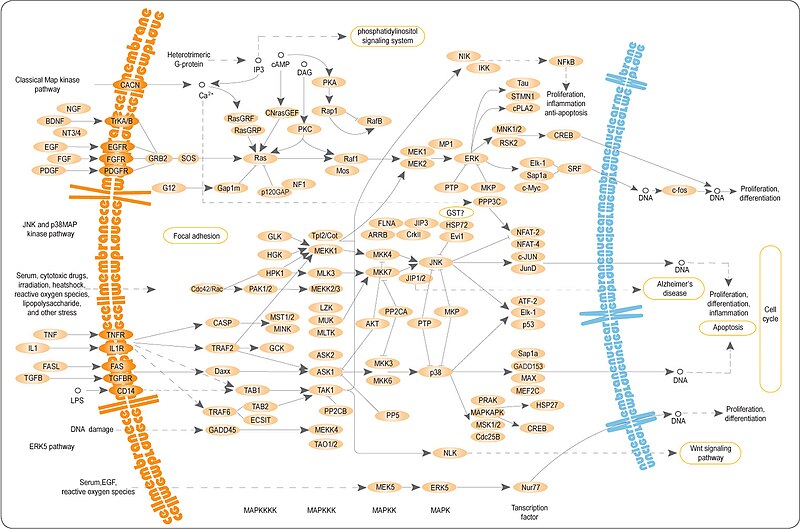
Genome profiling results showed a reduction in the nuclear abundance of NFkB 2.5 hours after massage, in parallel with reduced phopshorylation of HSP27 and IL-6 protein content.
In summary, these findings suggest that massage could contribute to an attenuated production of inflammatory cytokines which may reduce pain by similar mechanisms observed by conventional anti-inflammatory drugs. With this in mind, for sure there is a need of more studies using such techniques to understand more about the most effective massage protocols. Moreover, more is needed to understand when not to use massage. In fact, considering the possibility of such intervention of reducing the inflammatory response, one wonders the potential of such intervention to impair the adaptive responses to resistance exercise. Needless to say that more studies are needed using resistance exercise models and well trained individuals to ascertain the potential and the limitations as well as the contra-indications of massage therapy.





0 comments:
Post a Comment